Normal Pressure Hydrocephalus
Hydrocephalus is derived from the Greek: “hydro”-water and “cephalus” – head. Hydrocephalus usually results either from: 1) an imbalance between CSF production and absorption (communicating hydrocephalus); or 2) when there is a blockage within the ventricular system such as a tumor that prevents CSF circulation (obstructive hydrocephalus).
Adult communicating hydrocephalus is most commonly referred to as normal pressure hydrocephalus (NPH). However this is a misnomer, as the pressure may or may not be normal in a given patient. NPH usually occurs in older adults, with the majority of affected patients over 60 years of age. Most cases of adult communicating hydrocephalus/NPH are primary/idiopathic and of unknown cause. Some patients develop secondary NPH in association with or following subarachnoid hemorrhage, head injury, brain tumor, or meningitis.
Depending on the cause and type of hydrocephalus, a variety of neurosurgical interventions may be used for treatment.
Adult Communicating Hydrocephalus/Normal Pressure Hydrocephalus (NPH)
Symptoms
NPH has three primary symptoms:
- gait disturbance/imbalance
- urinary frequency/incontinence
- cognitive slowing/short term memory difficulty/dementia
Epidemiology
NPH is estimated to impact 0.5% of the population over 65 years old. However, this is likely an underestimate due to lack of recognition by patients and physicians unfamiliar with this condition.
Why is this a hard diagnosis?
Each of the primary symptoms has many other causes in the elderly population, and no combination of the cardinal symptoms is absolutely diagnostic.
The symptoms often develop slowly over a long period of time, and are mistaken for “normal aging”.
The ventricles enlarge with normal aging and with degenerative diseases such as Alzheimer’s disease.
All described diagnostic tests have false positives and negatives. No test is perfect in its ability to diagnose this condition.
|
Patient evaluation
1) Patients are evaluated by our multidisciplinary, experienced team composed of Movement Disorder Neurology, Cognitive/Aging Neurology, Neuroradiology, and Neurosurgery.
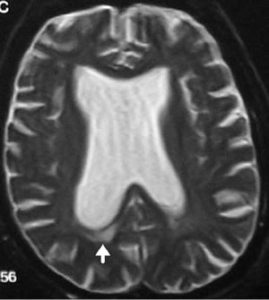
2) Patients who possibly have NPH based on their history and physical examination undergo brain imaging using MRI (CT scanning if pacemaker present). (See figure 1). Various sophisticating MR analyses help solidify the diagnosis of NPH.
3) All patients with possible of probable NPH are then evaluated with spinal fluid drainage to determine to what degree they improve with a test removal of spinal fluid. This testing is done in coordinated fashion between the Movement Disorder Neurology and Neurosurgery teams, using videotape analysis of gait function and cognitive testing before, during, and after spinal fluid drainage.Videotape analysis results in an unbiased Movement Disorder specialist determining to what degree function is improved by spinal fluid removal. This testing allows us to much better prognosticate whether a cerebrospinal fluid shunt implantation surgery will result in patient benefit.
While spinal fluid drainage is done as an outpatient is some certain circumstances via lumbar puncture (spinal tap), the majority of patients are admitted to the hospital of a spinal fluid lumbar drainage trial. A small catheter is placed into the lumbar (lower back) spinal fluid space, allowing spinal fluid removal over 2-3 days. In comparison with an outpatient spinal tap, inpatient lumbar spinal fluid drainage is more accurate and predictive of whether a shunt surgery will subsequently be of benefit.
Treatment
Ventricular shunt surgery: If a patient’s symptoms improve with spinal fluid drainage, a shunt surgery is offered to the patient (and family). The goal of a shunt is to divert CSF into another region of the body where it can be absorbed, such as the peritoneal (abdominal) cavity or int o a vein just above the heart. The shunt is a soft tube that is just over 2mm (less than 1/8 inch) in diameter. The synthetic shunt material is generally very well tolerated by the human body. The entire shunt is implanted either within the skull or under the skin. No components of the shunt are visible outside of the body. Between the shunt catheter in the brain and the catheter that goes to the abdomen or bloodstream, there is a one way valve that regulates CSF flow through the shunt. If there is too much flow, the ventricles will collapse and bleeding can occur. If there is too little flow, the patient’s symptoms will not improve.
All NPH shunts that we implant contain a magnetically programmable valve. This allows us to fine tune the shunt function over time to maximize patient safety and minimize complications. Shunt surgery is usually brief and safe. The shunt is implanted under general anesthesia in a procedure that takes about an hour. A small hole is made in the skull, and the membranes between the skull and brain are opened. The brain end of the shunt is gently passed through the brain into the lateral ventricle. The valve and abdominal (peritoneal) end is passed under the skin and then implanted into the abdominal cavity through a small abdominal incision. For venous shunts that are placed just above the heart, a percutaneous, minimally invasive technique is used.
Endoscopic third ventriculostomy: In some cases of adult hydrocephalus we are able to determine that there is a CSF blockage that can be potentially bypassed using an endoscopic surgery. In this type of shunt surgery, an endoscopic camera and microinstruments are manipulated through a minimally invasive, computer guided approach into the ventricle. A small hole is made in the floor of the third ventricle, allowing CSF to flow out of the brain. When successful, this type of surgery corrects the hydrocephalus without requiring a shunt implantation.
Results
Patients whose symptoms improve with spinal fluid drainage have a better than 80% chance of sustained improvement in gait function following implantation of a CSF ventricular shunt system. Improvement in cognition and urinary function is more variable, but occurs >50% of the time. A shunt is an implantable tube that allows the excess fluid to drain from the ventricles to other parts of the body for reabsorption. The exact type and location in the body of the ventricular shunt system is determined by the treating surgeon. Most NPH shunts are placed from the brain ventricle into the abdominal peritoneal cavity, although sometimes shunts are implanted into a large vein just above the heart using minimally invasive technology.
Complications
Due our surgical experience, careful patient evaluation, multidisciplinary approach, and expert Neuroanesthesia, our center has an overall complication rate in NPH shunt surgery of <5%. This is far better than the 10-25% rates reported in large series in the medical literature. Complications can include infection (1-2%), the need to revise or reposition a shunt (1-2%), seizures (<1%), anesthestic/medical complications (1-2%), brain hemorrhage (<1%) or abdominal injury (<1%). Major complications are exceedingly rare.
Longitudinal Follow-up
NPH requires long term follow up of shunt function to minimize complications and maximize benefits. Shunt valves often need to be reprogrammed over time to get the best clinical benefit in a given patient.
For more information on Adult Hydrocephalus, contact one of our doctors.